
Upright posture is a first class lever mechanical system, such as a teeter-totter or seesaw (1, 2).
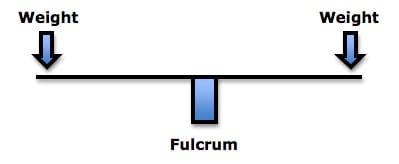
The fulcrum of a first class lever is the place where the force is the greatest: if excessively heavy objects are placed on both ends of the teeter-totter, it will break in the middle, at the fulcrum. In the spine, the fulcrum of the first class lever is the vertebra. Approximately 60% of weight is born by the vertebral body/intervertebral disc complex, and the other 40% is shared between the two facet joints. This means that when the first class lever of upright posture is altered, for any reason, there is an increased mechanical load born by the fulcrum, i.e. the spinal intervertebral discs and facet joints. Such increased mechanical loads accelerate degenerative joint disease (1, 3). In their 1990 book Clinical Biomechanics of the Spine (2), White and Panjabi state:
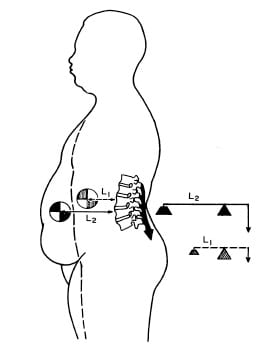
“The load on the discs is a combined result of the object weight, the upper body weight, the back muscle forces, and their respective lever arms to the disc center.”
Note the representative drawing from their text below; once again, the “Disc Load” is the fulcrum:
Classic events that alter the upright postural mechanical system include postural distortions, lifting ergonomics (1, 4), and weight problems (2). Weight problems are the primary point of this article.
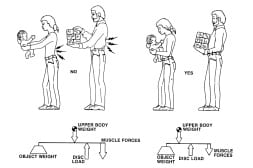
In their pioneering reference text Clinical Biomechanics of the Spine, Augustus White, MD, and Manohar Panjabi, PhD, also show (2) that when a person gains abdominal weight, the first class lever system of upright posture is altered in such a manner that the intervertebral disc and facet joints bear significantly more weight. To counterbalance the weight, the muscles on the other side of the fulcrum (spine) must constantly contract with more force, or the person would fall forward. The black arrow attached to the posterior spinal elements represents the muscle contraction.
This constant muscle contraction with more effort, creates muscle fatigue and myofascial pain syndromes. Rene Cailliet, MD states “This increase [in muscle tension] not only is fatiguing, but acts as a compressive force on the soft tissues, including the disk.” (1).
Obesity is linked to numerous health outcomes and disease risk factors, including hypertension, heart disease, stroke, cancer, diabetes, dementia, and arthritis. Simply stated, joints that have to bear more weight wear out at an accelerated rate. As noted by Drs. White and Panjabi, additional weight is not carried symmetrically; people tend to gain weight in their abdomen. This essentially is the equalivent of having a “heavy kid” on one end of the teeter-totter. To balance, the muscles on the opposite side of the fulcrum (the posterior paraspinal muscles) must increase their tension or the subject would fall forward onto their face.
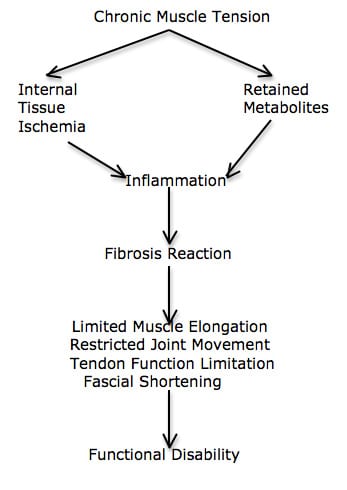
Rene Cailliet explains how the constant contraction in the counterbalancing muscles creates a cascade that leads to muscle fatigue, inflammation, fibrosis, and eventually to chronic musculoskeletal pain syndromes (5):
It is the accelerated degeneration of the spinal discs and facet joints (the spinal fulcrum) that are of particular important concern.
•••••••••
The classifications of being overweight or obese are based on a person’s Body Mass Index (BMI). The BMI is calculated using pounds and inches using this formula (6):
[(weight in pounds) / (height in inches X height in inches)] X [703]
As an example, a 6 foot (72 inches) person weighing 200 pounds:
[(200) / (72 X 72)] X [703] =
[(200) / (5184)] X [703] = 27.1 (overweight, see below)
It is not necessary to do this math in calculating a person’s BMI; one can simply go to countless web pages on the internet and there are available free BMI calculators. All one has to do is plug in their numbers and the math is automatically done.
Although the BMI is controversial, it is still used in assessing weight issues, as follows:
18.5 – 24.9 Normal
25.0 – 29.9 Overweight
30.0 – and up Obese
40.0 – and up Severely Obese (more than 100 pounds overweight)
Our nation was stunned when official tabulations indicated that 69% of American adults are overweight or obese (7). The national shock deepened when these numbers were soon revised, predicting that these rates would essentially double in the next 17 years, by 2030 (8). In our heaviest state, Mississippi, it is estimated that by 2030, 67% of adults will be obese (8). Economically, Mississippi is also our poorest state, attesting to the irony that our economically poorest state is also our heaviest. The national disbelief continued when it was understood that severe obesity rates (BMI over 40, which is more than 100 pounds overweight) is skyrocketing (9).
•••••••••
Is there a link between poverty and weight gain? What is happening to cause such extreme weight gain in our population?
•••••••••
Obesity rates affect chiropractic clinical practice in a number of ways. The most obvious is that obesity increases degenerative joint disease of weight bearing joints, including the disc and facets of the spine. These changes are chronic and often linked to chronic pain syndromes; they are often debilitating. There is no “cure” for the joint destruction.
Science writer Gary Taubes expresses a leading theory explaining America’s skyrocketing obesity rates. Educated at Harvard and Stanford, Taubes is currently a Fellow at the University of California, Berkeley. His recent writings on the obesity topic include Good Calories, Bad Calories (2008) (10), Why We Get Fat (2011) (11), and the cover article in the political magazine Newsweek (5/14/12) (12).
Taubes presents compelling evidence that obesity is linked to insulin. The more insulin produced in response to a consumed food (insulin response), the fatter the person becomes. The insulin response to a consumed food is called the Glycemic Index.
Taubes first book on this subject, Good Calories, Bad Calories (2008), presents 600 pages of compelling and often complex physiology and evidence in explaining the insulin-obesity connection. Perhaps the key premise, although grossly oversimplified, is as follows:
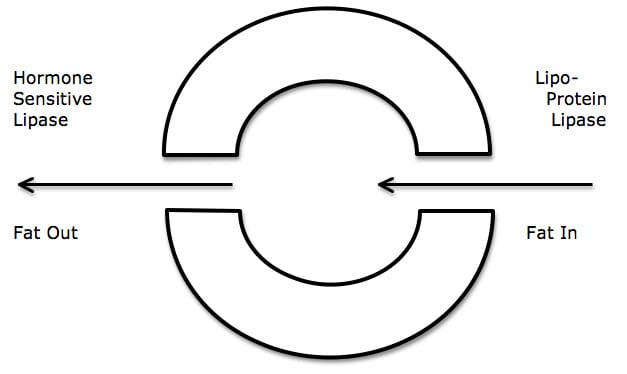
- Fat cells become fatter when more fat enters the cell than leaves the cell.
- The “door” that lets fat into the cell is controlled by an enzyme called lipoprotein lipase.
- The “door” that lets fat leave the cell is controlled by an enzyme called hormone sensitive lipase.
- Both enzymes (lipoprotein lipase and hormone sensitive lipase) are controlled by insulin.
- Insulin up-regulates the production of lipoprotein lipase. This opens the “door” to the fat cell and more fat enters the cell. The fat cell becomes fatter.
- Insulin down-regulates the production of hormone sensitive lipase. This means that the “door” that lets fat out of the fat cell is closed, and the fat cannot escape.
- The fat cell can only hold so much fat. When capacity is reached, the cell responds by dividing, doubling the number of fat cells.
- With continued exposure to insulin, the process continues. As biochemist Dr. Barry Sears says (13):
“It is excess insulin that makes you fat and keeps you fat.”
In his 2009 book The End of Overeating, Physician David Kessler, MD, presents a remarkable discussion pertaining to human dietary habits (14). Dr. Kessler is the former FDA (Food and Drug Administration) commissioner, holding the job for both presidents George HW Bush (1990) and Bill Clinton. Dr. Kessler is a Harvard educated pediatrician, and also holds a law degree from the University of Chicago. Dr. Kessler’s book integrates anthropology, biology, biochemistry, neurology, neurophysiology and physiology. His basic premise is that humans evolved with neurophysiological addictions that help to ensure the survivability of the human species. These addictions primarily center on sex and the neurotransmitter dopamine: humans are biologically addicted to dopamine; thinking about sex and participating in sex increases the production and release of dopamine. Humans are addicted to the pleasurable sensations attributed to this dopamine release.
Experiences other than sex can also increase the production and release of dopamine. Consequently, these experiences are also addicting. Examples include illegal drugs like cocaine, chocolate, and sadly, refined carbohydrates that have a high Glycemic Index.
If one is addicted to the increased production and release of dopamine as a consequence of the consumption of high Glycemic refined carbohydrates, one will constantly consume such foods, often not understanding that their consumption and overconsumption is actually a brain neurochemical addiction. Such habits constantly elevate systemic insulin levels. Lipoprotein lipase enzyme up-regulation pushes fat into the fat cells. Hormone sensitive lipase shuts the “door” so that the fat cannot escape. The person becomes fatter.
In his 2011 book The Sugar Barons, Matthew Parker indicates how the sugar barons of centuries ago exploited this human sugar-refined carbohydrate-dopamine addiction to become fabulously wealthy (15). Apparently, contemporary food producers and suppliers are continuing this exploitation. A few hundred years ago the typical American consumed 5 pounds of sugar. Today average sugar consumption is 160 pounds per American per year (16).
•••••••••
In 1968, America was at the height of the Vietnam War. Protesters and rioters were dogging the Democratic National (presidential) Convention in Chicago. The population of planet earth was about 3.5 billion people. And a Stanford University Professor named Paul Ehrlich wrote a book titled The Population Bomb (17). Paul Ehrlich (born May 29, 1932) is an American biologist and educator who is the Bing Professor of Population Studies in the department of Biological Sciences at Stanford University and president of Stanford's Center for Conservation Biology. His book is subtitled:
“Population Control or Race to Oblivion”
“While you are Reading These Words, Four People will Have Died from Starvation. Most of them Children.”
Dr. Ehrlich’s prediction of mass human starvation as a consequence of exploding human populations never happened. Apparently, Dr. Ehrlich did not know that a man was already on the job of preventing such a disaster, and had been working on the solution since 1944. Norman Borlaug was plant biologist and geneticist from the University of Minnesota. Paul Ehrlich was not up on Borlaug’s research. Through genetic manipulation and the use of powerful synthetic fertilizers, Borlaug was able to significantly increase crop yields. His efforts and success at feeding the world earned him the Nobel Peace Prize in 1970, two years after Paul Ehrlich’s book came out. Norman Borlaug died in 2009 at age 95. The human population has doubled, to 7 billion people.
There is concern that Norman Borlaug’s successes may be temporary, having delayed the inevitable. Paul Ehrlich certainly believes as much. Also, Borlaug’s farming methods have created other ecological disasters: damage done by chemical runoff from tons of synthetic fertilizers pollute waterways around the globe and create huge “dead zones,” where no living thing can exist.
Another consequence of Norman Borlaug’s genetic manipulation is important for this article: obesity. People around the world, even our most poor, are gaining weight at an alarming rate. A detailed explanation for this phenomenon is found in the 2011 book Wheat Belly, by cardiologist William Davis, MD (18).
Dr. Davis explains that the unique genetic manipulation of wheat by Norman Borlaug included a process of chromosomal addition called polyploidy. This resulted in a new modern wheat that is 90% carbohydrate. Sadly the carbohydrate in this new wheat is called amylopectin-A, a carbohydrate that has an extremely high Glycemic Index. Although Norman Borlaug’s efforts resulted in increased crop yields, improved harvesting efficiency, and desirable palliative and baking aesthetics, modern wheat’s high Glycemic Index is being linked to obesity and all of its related health problems (hypertension, heart disease, stroke, cancer, diabetes, dementia, arthritis, etc.). Dr. William Davis states:
“The amylopectin-A of wheat products, complex or no, might be regarded as a super-carbohydrate, a form of highly digestible carbohydrate that is more efficiently converted to blood sugar than nearly all other carbohydrate foods, simple or complex.”
Obesity is a global problem. Internet searches indicate that global consumption of wheat is presently 356,218 thousand metric tons per year (19). World trade in wheat is greater than for all other crops combined. Dr. Davis ends his book with this question:
“This idea that wheat is not only making people ill, but killing some of us—some quickly, others more slowly—raises unsettling questions: What do we say to the millions of the people in Third World countries who, if deprived of high-yield wheat, might have less chronic illness but greater likelihood of near-term starvation? Should we just accept that our far-from-perfect means justifies the net reduced mortality end?”
•••••••••
SOLUTIONS
Losing weight is never easy. I prefer to make a custom program for my patients based upon specifics of their lives and habits and health. However, I use these three strategies on all of our overweight patients. They are simple and effective:
- Do not eat refined carbohydrates; this is the most important rule: Sugary drinks including juice, all sugary foods, breads, pastas, potatoes, rice.
- Do not consume grains because they are carbohydrates. The worst grain is wheat, even whole wheat, because of its high Glycemic Index amylopectin-A.
- Do not drink your calories.
Dr. Barry Popkin is a distinguished Professor of Global Nutrition at the University of North Carolina. In his 2009 book titled (20), he notes:
The World Is Fat The Fads, Trends, Policies, And Products That Are Fattening The Human Race
“The world has become fat in just a few decades.”
“Ultimately, widespread obesity and the chronic diseases that contribute to the bulk of deaths in the world are less a result of poor individual dietary choices than the consequences of a high-tech, interconnected world in which governments and multinational corporations have extraordinary power to shape our everyday lives.”
“Man ate and drank in the healthiest manner possible during the Upper Paleolithic period [beginning about 40,000 years ago], when humans were nomadic hunter-gatherers.” “About 50%-80% of food came from plants and 20%-50% from animals.” “People living at this time consumed no grains, and no dairy products other than breast milk.”
“So, on one hand, we have much cheaper beef, poultry, corn, soybeans, and sugar. But on the other, this has occurred at the expense of healthy plant foods—particularly fruits and vegetables, whose relative cost is great compared to [subsidized] fats, sugars, and meats in today’s marketplaces. The results for all of us—not only American but around the globe—have been devastating.”
“Today, we’re awash in highly refined sugar and grains.”
“Nothing has contributed more to our weight gain than the clash between our drinking habits and our biology.” “We drink a lot of our calories, but we don’t cut our food intake as a result.” “The average American gets over 450 calories a day from beverages.”
“My [Popkin] favorite way to help people lose weight is to look at what they drink over the course of a typical day.” “The top 40% of caloric beverage drinkers in the US consume over 760 calories a day from beverages.” “It would be difficult for a person to be heavy if he or she drank only water, consumed a small amount of added sugar in foods, ate lots of fruits and vegetables, and ate no fried foods. Of course, one needs also to be physically active.”
Nutrition expert Marion Nestle from New York University agrees with Dr. Popkin, stating in her 2012 book Why Calories Count (21):
“Don’t Drink Your Calories”
Both Dr. Popkin and Dr. Nestle indicate that satiety comes from eating, not drinking. If one eliminates calories from drink, food intake will not increase. The reduced calories from not drinking them will cause weight loss, and the patient will not feel hungry, they will still achieve satiety.
Even modest loss of weight significantly helps in the management of our musculoskeletal patients.
REFERENCES
- Cailliet R; Low Back Pain Syndrome, 4th edition, F A Davis Company, 1981.
- White AA, Panjabi MM; Clinical Biomechanics of the Spine, Second Edition, Lippincott, 1990.
- Garstang SV, Stitik SP; Osteoarthritis; Epidemiology, Risk Factors, and Pathophysiology; American Journal of Physical Medicine and Rehabilitation; November 2006, Vol. 85, No. 11, pp. S2-S11.
- Oschman J; Energy Medicine; Churchill Livingstone; 2000.
- Cailliet R; Soft Tissue Pain and Disability; 3rd Edition; F A Davis Company, 1996.
- Mercola J; Sweet Deception; Nelson Books; 2006.
- Hellmich N; Obesity rate may hit 42% by 2030; USA Today; May 8, 2012.
- Hellmich N; State obesity rates could soar by 2030; USA Today; September 19, 2012.
- Hellmich N; Percentage of severely obese adults skyrockets; USA Today; October 2, 2012.
- Taubes G; Good Calories, Bad Calories: Challenging the Conventional Wisdom on Diet, Weight Control, and Disease; Anchor Books; 2008.
- Taubes G; Why We Get Fat and What to do About It; Anchor Books; 2011.
- Taubes; “The new obesity campaigns have it all wrong”; Newsweek; 5/14/12; pp. 32-36.
- Sears B; Toxic Fat: When Good Fat Turns Bad; Thomas Nelson; 2008.
- Kessler D; The End of Overeating, Taking Control of the Insatiable American Appetite; Rodale; 2009.
- Parker M; The Sugar Barons: Family, Corruption, Empire, and War in the West Indies; Walker & Company; 2011.
- O’Connell J; Sugar Nation: The Hidden Truth Behind America’s Deadliest Habit and the Simple Way to Beat It; Hyperion; 2010.
- Ehrlich P; The Population Bomb; Sierra Club; 1969.
- Davis W; Wheat Belly; Rodale; 2011.
- http://www.nationmaster.com/graph/agr_gra_whe_con-agriculture-grains-wheat-consumption.
- Popkin B; The World Is Fat: The Fads, Trends, Policies, And Products That Are Fattening The Human Race; Avery, 2009.
- Nestle M, Nesheim M; Why Calories Count, From Science to Politics; University of California Press; 2012.

